


How has your salary changed since the start of the pandemic?

Although I am one of an estimated 2.7 to 3 per cent of the population that meets the Centers for Disease Control (CDC) definition of “immunocompromised,” I am in a position of privilege. This is because a) I’ve managed to avoid getting COVID-19 so far – knock on wood – and b) thanks to those four Moderna jabs, my body is generating an antibody response.
Whether or not said antibody response is sufficient remains unclear. According to my understanding there is no comprehensive guidance on how to differentiate between sufficient antibody responses and insufficient ones but because I am in dialog with immunocompromised people who do NOT generate an antibody response to the vaccine I know my response is the preferred one. I also wish more comprehensive data and data assessment tools were available.
Thanks to the “Immunocompromised People are not Expendable” support group founded by patient advocate and activist Michelle Burleigh, along with a hard-working team of volunteer admins who vet members, I have been able to learn a lot. We share articles, resources and impressions of what supports systems —or lack of them— are like where we live. At the beginning of 2022 when I decided to launch a newsletter for the community I began, with the groups permission and encouragement, running surveys to figure out what to write about. It is thanks to their support and feedback that I am able to launch Immunocompromised Times, a newsletter for people who meet the CDC’s definition of “moderately to severely immunocompromised,” as well as their friends, family members and allies.
I myself meet this CDC definition because of Remicade. Remicade, the Johnson and Johnson medication I take to manage Crohn’s disease, has kept my Crohn’s in remission since 2007. Remission did not come about on its own, and it did not come about due to Remicade. My Crohn’s at the time was severe enough to necessitate the surgical removal of six inches of ulcerated small intestines.
Upon finally being released from chronic and sometimes debilitating pain, massively inconvenient monthly three-to-10-day hospitalizations and, in some cases, unanticipated claim denials for medically necessary services that my then pre-Obama-era private health insurance refused to pay, I went on Remicade to manage occasional post-surgical flares and maintain my remission.
Up until now, the disadvantages of publicly sharing my experiences with Crohn’s disease has always outweighed the advantages. As we close out year two of the pandemic and enter year three, however, the things I’ve always feared going public about – the challenges and complexities of living in a country that marginalizes and devalues people with chronic medical conditions – are coming to pass anyway.
Crohn’s is rarely terminal, thanks to the kinds of pharmaceutical and surgical interventions I’ve had the benefit of receiving. I have relatively few restrictions, other than the occasional dietary ones like not being able to eat popcorn or granola. Remicade restrictions that didn’t used to be an issue for me now take center stage, and there is absolutely no way to avoid discrimination on the grounds of something that, until recently, many people didn’t even know existed. Immunocompromised Times is addressing this in the inaugural issue in an effort to fill one of many gaps in news coverage.
Although Immunocompromised Times’ primary audience is the people who meet the CDC definition of moderately to severely immunocompromised and their allies, future issues of this newsletter will have relevance to people with autoimmune diseases who have chosen to go off immunosuppressants, as well as members of the general population who simply want to avoid getting COVID. It will cover things like risk assessment, makeshift safety hacks and strategies for stealing positivity when life in the Kafka-ville or, depending on metaphoric genre preferences, the zombie apocalypse starts to get you down.
The results of the small survey I took to compare responses from people in the vetted “Immunocompromised People are not Expendable” support group are contrasted to survey responses reported by people I know in real life (as opposed to just virtual social media interactions) and who I can send follow up questions to, if need be.
The immunocompromised group survey was done in a Facebook group using the “poll” feature (I put “poll” in quotes to emphasize this was not scientific enough to meet the technical definition of poll. The data could have also been affected by the fact everyone could what the others wrote in response.
The immunocompetent group, by contrast, was done using Google sheets. The survey I created for the immunocompetent group did not show results to anyone other than me and the people responding to them. Google sheets also enabled me to capture people’s names, responses and follow up information so that a third party who wants to review my process and/or try to replicate the results can do so. Were I to replicate the survey I dispense with the inaccurately titled Facebook “poll” and do all my research using Google sheets.
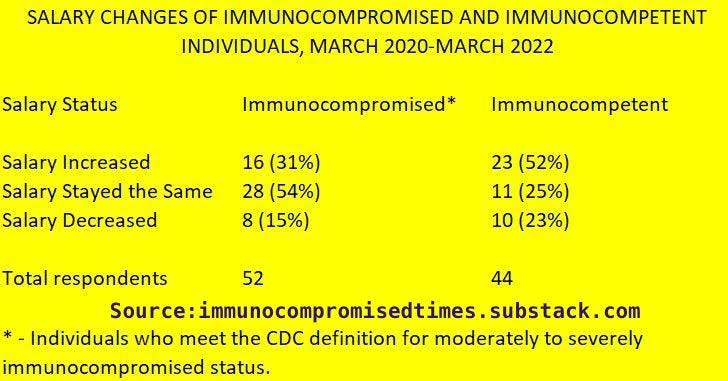
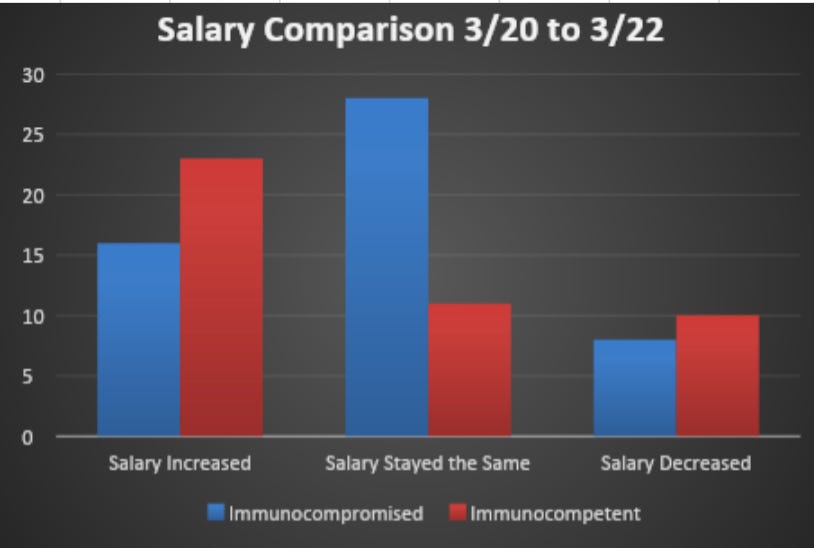
The data are posted here in chart and graph format to make it easy to compare and contrast the immunocompromised and immunocompetent groups while reflecting on your own salary and income changes over the last two years.
Like many issues Immunocompromised Times posts will delve into, more information is needed to draw substantial conclusions but this is a start.
What other data sets shall I try and track down for you?